
What is Palliative Care?
Common Misconceptions About Comfort, Treatment, Hospice, and Serious Illness
For many people palliative care, sounds like a door closing. It can sound like the end of treatment, that there’s no hope, or that proverbial moment when a doctor says, “There’s nothing more we can do for you.”
But palliative care is not a closed door.
It is neither the absence of care nor the absence of treatment. It is also not just for the final weeks and days of life. It’s about living the best quality life for as long as possible.
At it’s core, palliative care is whole-person care for someone living with serious illness. It focuses on comfort, pain and symptom relief, quality of life, clear communication, emotional and spiritual support, and helping people and families navigate difficult decisions with clarity and less fear. Health Canada describes palliative care as a holistic approach for people with serious illness, of any age and in any setting. It involves a range of care providers, including a person’s unpaid family members and caregivers.
Why is Palliative Care so Misunderstood?
These misconceptions exist for very understandable reasons.
For many people, palliative care is brought up late in an illness, when someone is already declining or nearing the end of life. By then, it feels very final. Even though palliative care can be introduced much earlier, many people associate it with dying.
We also live in culture that equates “good medical care” with fixing, curing, interventions, and extending life. Those things are important – and made possible by important, game-changing advancements in medicine – but when the focus shifts towards comfort, quality of life, symptom relief, and support, it can be mistaken for “giving up the fight”.
Part of the misunderstanding could also be that palliative care is still relatively new as a medical specialty compared to other areas of medicine. In Canada, the term “palliative care” was coined in 1975, but it wasn’t until 2013 when it was formally recognized as a 2-year subspecialty by the Royal College, after being gradually developed over decades.
This misunderstanding doesn’t only exist among the general public. Research shows that even healthcare professionals can have gaps in understanding palliative care – including when it’s appropriate, who it’s for, and whether it applies beyond end-stage cancer care.
So if you feel confused by the term, you are definitely not alone. The language itself is loaded and even the healthcare system doesn’t always thoroughly explain what palliative care really is.

Palliative Care is Both a Specialty and an Approach to Care
Palliative care can be a medical specialty involving physicians, nurses, social workers, pharmacists, occupational therapists and other trained professionals.
But it can also be an overall approach or attitude to care that is adopted by any healthcare provider throughout a person’s illness. A palliative approach asks questions like: What symptoms are causing pain and distress? What matters the most to this person? What does quality of life mean to them? What supports do the family or caregivers need?
In other words, palliative care looks beyond the disease and sees the whole person in the fuller context of their life.
Palliative Care is Not Just for the End of Life
A very common myth is that palliative care is only brought in when someone is very close to death. What people don’t recognize is that it can begin much earlier – sometimes even at diagnosis – especially if someone is facing a serious, progressive, or life-limiting illness.
A person does not have to be “terminal” to benefit from palliative care. They may be living with cancer, dementia, heart disease, lung disease, neurological illness or another serious condition. Palliative care is not based on proximity to death, but rather the person’s unique needs, quality of life, and overall experience of living with serious illness.
It can also be provided in many settings including the home, hospital, long-term care, and hospice. It is not defined by the location, but rather the focus of care.
Palliative Treatment can Happen Alongside Curative Treatment
Palliative care doesn’t mean that treatments have stopped. It means that the goal of treatment is different. Some treatments are aimed at curing or reversing a disease, while others are intended to reduce pain, relieve symptoms, improve function, or enhance quality of life.
For example, a person with advanced cancer may receive palliative radiation not because it’s expected to cure the cancer but because a tumour is causing pain, pressure, difficulty swallowing or breathing. A person may have surgery to ease symptoms, such as relieving a blockage. The goal may not be to cure the underlying illness, but it is still treatment.
Palliative treatment can also happen alongside curative forms of treatment. Somebody might be receiving chemotherapy, dialysis, cardiac treatment, surgery, while also getting palliative care for symptoms such as nausea, pain, breathlessness, anxiety, sleep issues, and more.
This is why palliative care shouldn’t be framed as “nothing more can be done.” Whether it is offered alongside curative treatment or when curative options are no longer effective, there is still so much that can be done to care for the whole person, ease suffering, and preserve quality of life.
Palliative Care vs Hospice. What’s the Difference?
This is one of the biggest misconceptions. A simple way to think about it is that palliative care is the umbrella term under which hospice falls. Or, all hospice care is palliative care, but not all palliative care is hospice care.
Hospice care focuses on comfort and support when it’s been determined that a person is nearing the end of life. Eligibility and timing can vary depending on the program, location, and individual situation. Palliative care is broader and can start much earlier and continue alongside other types of care, as previously discussed.
This distinction is important because when people think of palliative care, their mind jumps to hospice care, and they may resist palliative support because they mistakenly believe that it’s premature.
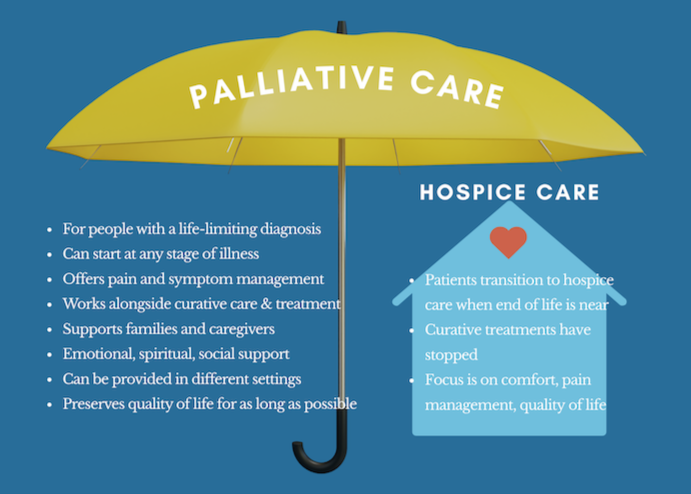
The Palliative Care Umbrella
How to Ask for a Palliative Approach
You don’t have to wait for a healthcare provider to bring up palliative care. And not every clinician – unless they are specifically a palliative care provider – will automatically work with a palliative mindset.
That’s not because they don’t care, but many healthcare providers are trained to diagnose, fix, treat, intervene, and prolong life whenever possible. This kind of care can save lives and be deeply valuable.
But serious illness also requires conversations about comfort, values, acceptable trade-offs, emotional well being, quality of life, family support, and what matters the most to the patient.
A palliative approach broadens the conversation and sometimes it needs to be invited to the table. Some helpful language to start that discussion might be:
“Can we talk about quality of life, not just treatment options?”
“I’d like to talk about involving palliative care for managing my symptoms.”
“Can I also get a palliative care referral while I’m receiving this treatment for extra support with planning ahead?”
These types of questions can open the door for better support, clearer communication, and more person-centred care. It can also make a patient feel more agency within their illness journey.
Palliative Care Needs a Better Public Conversation
Part of the challenge is that the term palliative care instills a lot of fear and resignation in people. It sounds like the end stage, not the broad web of support that it is.
What if we understood it to be not only end-of-life care, but as holistic, person-centred care focused on comfort, quality of life, and support during serious illness?
Changing the perception of palliative care isn’t just the domain of healthcare providers. It can be a cultural conversation. We can help shift the meaning by asking better questions, sharing clear information, and refusing to reinforce an outdated understanding that comfort equates to giving up. Palliative care is not about abandoning hope; it’s about expanding care.
When we understand it that way, people and their families may be more willing to accept and receive the support need earlier, so they have a better experience throughout their illness journey, not just at the end.
Final Thoughts
The more we understand what palliative care is, the less frightening it is. And the sooner people and families can access this type of care, the less alone they will feel as they navigate illness, caregiving, uncertainty and change.
Palliative care isn’t about giving up. It’s about making sure the whole person is cared for – not just their illness, but their personhood, their choices, their relationships, and their quality of life.
If you or a loved one is living with serious illness and you’re looking for non-medical support, education, or help beginning conversations about comfort, care wishes, and what matters most, I’d be honoured to support you. Reach out to me anytime.
Thank you for being here.
Sarah xx